
In a hospital with multiple branches, radiology reporting is often the thread that binds decisions across locations. Yet when each branch follows different reporting styles, inconsistencies arise that can affect both diagnosis and patient confidence. For decision-makers, the challenge is not just about producing reports, but about ensuring that every report, whether generated in a metropolitan branch or a district unit, speaks the same language of clarity and precision.
Multi branch radiology therefore demands a system of uniformity. Without it, even the best imaging can lose its value in communication gaps. By adopting structured reporting, standardized templates, and integrated RIS–PACS systems, hospitals can achieve consistency across all sites. The outcome is better collaboration, improved patient trust, and stronger clinical decision-making.
The Challenges of Multi Branch Radiology
Operating radiology services across several branches is not without hurdles. While imaging hardware may be standardized, the way radiology reports are written, moved through RIS–PACS workflows, and acted on can vary widely. These variations create friction for referring clinicians, slow cross-site collaboration, and introduce avoidable risk. A focused path to consistency starts by understanding where discrepancies originate and how to correct them with policy, software, and training.

3 Challenges of Multi-branch Radiology
1. Variations in Reporting Formats
A CT chest from Branch A might list long-form “ground-glass opacities,” while Branch B writes “GGO” and places incidental findings above critical impressions. Such differences force clinicians to re-interpret structure before reading content. Standardization means defining mandatory sections (Indication, Technique, Findings, Impression), agreed terminology, and consistent laterality/time-comparison language so every site “sounds” the same.
- Adopt structured templates with fixed headings and picklists for common studies.
- Maintain a shared terminology/glossary (e.g., expand abbreviations, unify descriptors).
- Lock critical fields (Impression first; urgent items flagged) to protect order and clarity.
For instance, when a stroke MRI template enforces Impression-first with NIHSS context, emergency teams across branches act faster with fewer clarifications.
2. Limited Interoperability Between RIS and PACS
When RIS and PACS are loosely connected, prior studies from another branch may not appear in the same worklist, or patient IDs don’t reconcile. Radiologists then chase data, duplicate uploads, or read without priors, direct hits to quality and turnaround. Interoperability is achieved by unifying patient identity, accession formats, and viewer access so images, priors, and reports travel together.
- Enforce a single patient master index and consistent accession numbering across branches.
- Integrate RIS–PACS with HL7/DICOM routing so priors auto-attach to new studies.
- Provide a cloud/zero-footprint viewer with role-based access for all sites.
Example: A neuroradiologist at HQ opens a Branch B MRI and instantly sees Branch A’s prior CT and report in one pane, no re-requests, no delays.
3. Human Workflow Differences
Even with templates, individual habits persist: one radiologist dictates free text; another overuses shorthand; a third rearranges sections. Over time these micro-variations erode the consistency that multi branch radiology needs. The remedy is governance plus coaching — clear SOPs, routine audits, and feedback loops that help teams converge on a common reporting “voice.”
- Publish site-wide SOPs and a reporting style guide; onboard every new radiologist to both.
- Run periodic peer review/QA audits with targeted feedback and exemplar reports.
- Use analytics from the reporting system to spot deviation (missing fields, section order).
For example, monthly audits can flag branches where “Technique” or “Comparison” is frequently absent, prompting quick retraining and template tweaks.
Key Systems for Standardized Reporting
Consistency in multi branch radiology is impossible without strong backbone systems. Even the most skilled radiologists need a unified digital environment that allows them to access, interpret, and report studies the same way across every branch. The cornerstones here are RIS, PACS, and cloud-based platforms, which together form the framework for standardization.
1. RIS (Radiology Information System) for Data Consistency
The Radiology Information System (RIS) is where reporting begins. It manages patient demographics, study orders, scheduling, and report documentation. Without RIS standardization, each branch may record studies differently, creating fragmented data trails. A centralized RIS ensures that patient identifiers, study descriptions, and reporting templates are consistent across all locations.
- Enforce a shared RIS database or connected instances across branches.
- Configure uniform templates for exams (e.g., CT brain, chest X-ray, MRI spine).
- Map codes and fields so referring physicians always see identical formats.
For example, a neurologist comparing CT reports from two different branches can quickly spot changes without decoding different layouts or terminologies.
Radiology Information System
2. PACS (Picture Archiving and Communication System) for Imaging Access
PACS stores and retrieves images, but its role in multi-branch settings goes beyond archiving. If each branch runs a siloed PACS, radiologists cannot access priors, leading to incomplete interpretations. A unified PACS ensures that historical imaging is available instantly, no matter where the patient was first scanned.
- Implement a single enterprise PACS or vendor-neutral archive (VNA).
- Standardize DICOM tags to avoid mismatched or orphan studies.
- Provide universal worklists that pull cases from all branches into one queue.
For example, when a patient undergoes an MRI in Branch B but returns to Branch A for follow-up, the radiologist sees both sets in the same viewer, ensuring accurate comparison.
PACS for Imaging Access
3. Cloud PACS for Inter-Branch Collaboration
Traditional PACS often limit access to local networks, slowing down collaboration. Cloud PACS removes this barrier by enabling radiologists, regardless of branch, to securely access images and reports from any location. For multi-branch hospitals, this means real-time sharing and uniform reporting workflows.
- Use a HIPAA-compliant or regionally approved cloud PACS to maintain data security.
- Enable zero-footprint viewers for radiologists to log in from different branches.
- Allow structured reporting modules within the cloud system to keep formats consistent.
For example, a subspecialty radiologist in the main hospital can review a rare pediatric case from a smaller branch without delay, ensuring both quality and consistency.
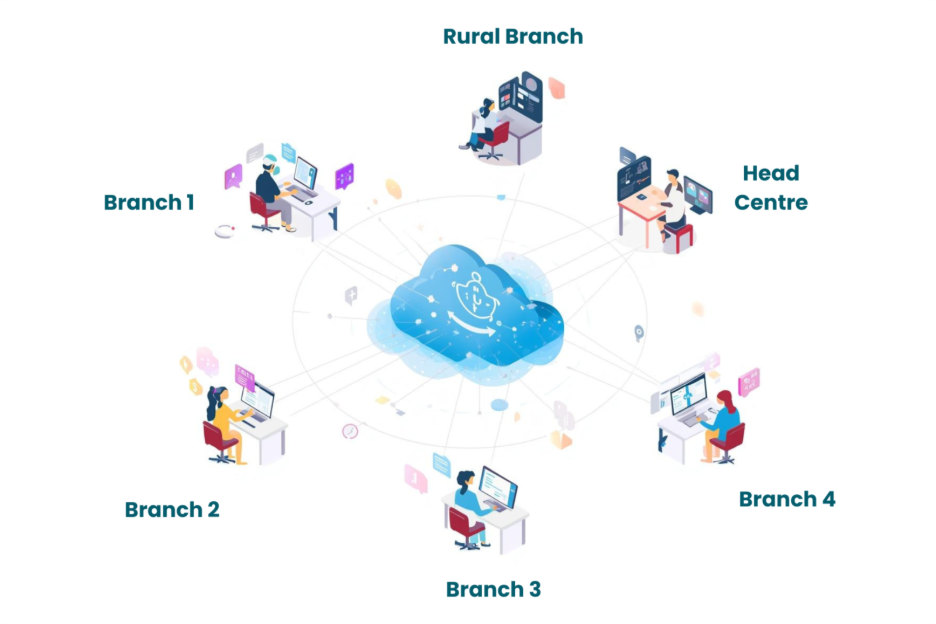
Collaboration amongst branches with cloud PACS
Strategies to Maintain Consistency in Radiology Reporting
Once the backbone systems are in place, the next step is applying strategies that ensure every radiology report coming out of a multi-branch network looks and reads the same. These strategies blend process, technology, and governance, and when applied together, they eliminate the confusion that often arises from fragmented reporting styles.
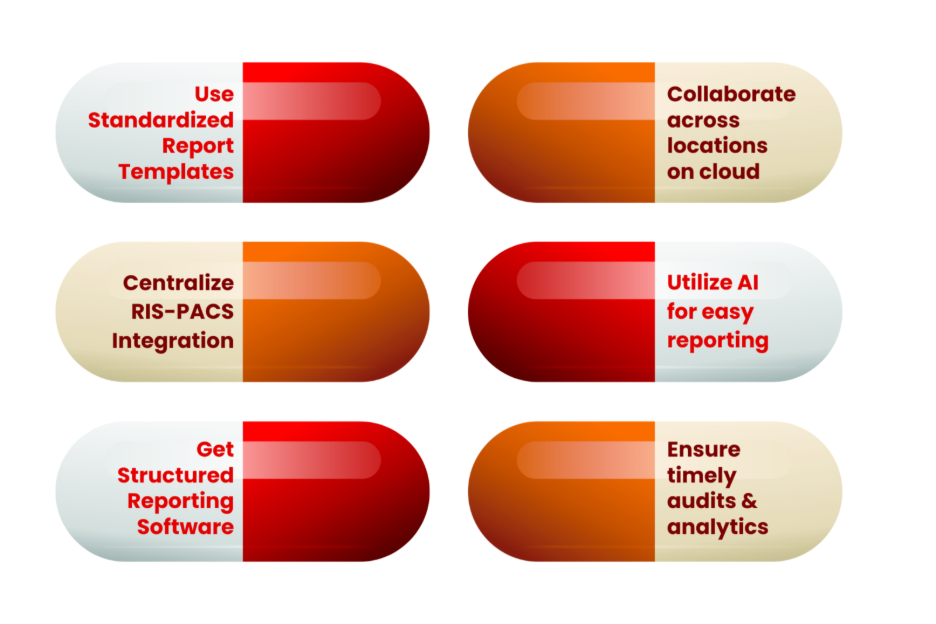
6 Strategies to maintain Consistant Reporting
1. Using Standardized Report Templates
Consistency begins with templates. Structured templates divide reports into fixed sections such as Indication, Technique, Findings, and Impression. This minimizes variation in how radiologists present information, especially when cases are handled across different branches.
- Define mandatory sections for all study types.
- Use standardized terminology for common conditions.
- Provide auto-filled fields for measurements and normal findings.
Example: A chest X-ray report template that auto-lists “heart size, lung fields, mediastinum” ensures uniform reporting even when multiple radiologists contribute.
2. Centralized RIS-PACS Integration
When RIS and PACS are fully integrated across sites, reporting becomes both uniform and faster. Radiologists see priors, orders, and patient data in a single interface, reducing errors from manual reconciliation.
- Enforce integration so reports are tied directly to imaging studies.
- Standardize patient IDs and accession numbers across branches.
- Provide radiologists with a unified worklist across locations.
For instance, instead of manually searching priors from another branch, a radiologist sees all relevant studies automatically attached in one viewer.
3. Structured Reporting Software for Radiologists
Free-text reports vary widely by radiologist. Structured reporting software solves this by guiding radiologists through dropdowns, checkboxes, and pre-defined fields. This enforces consistency without limiting clinical judgment.
- Implement reporting modules with structured data capture.
- Allow quick customization to meet subspecialty needs (neuro, chest, musculoskeletal).
- Train radiologists to balance structured fields with free-text where necessary.
Example: A stroke MRI report completed in a structured template ensures uniform documentation of infarct size, side, and severity across branches.
4. Cloud-Based Collaboration Across Locations
Cloud platforms ensure that all radiologists, regardless of site, can access reports and imaging in real time. This prevents “branch silos” where reports remain locked to one location.
- Adopt secure cloud PACS with real-time reporting access.
- Enable role-based permissions for consultants and trainees.
- Support cross-branch peer review through cloud viewers.
For example, a senior radiologist in the central branch can review and finalize reports from satellite branches instantly, preserving a uniform standard.
5. Leveraging AI and Automation for Consistency
Artificial intelligence in radiology is no longer futuristic; it plays a key role in standardization. AI can draft routine reports, highlight urgent findings, and enforce consistent terminology. Automation further reduces human variation by ensuring structured fields are never skipped.
- Deploy AI-driven draft reporting for high-volume studies like X-rays.
- Use natural language processing (NLP) to standardize terminology.
- Automate critical alerts (e.g., stroke, pulmonary embolism) for uniform flagging.
For instance, AI-generated chest X-ray drafts pre-fill “normal heart size, clear lung fields” where applicable, saving time while keeping format identical across branches.
6. Best Practices: Audits, Training & Terminology Governance
Technology alone is not enough. Consistency requires governance, active policies that guide and correct radiology practice.
- Conduct routine audits across branches to spot inconsistencies.
- Establish a style guide for report terminology and abbreviations.
- Train radiologists and junior doctors on the reporting standards during onboarding.
Example: A monthly audit may reveal that Branch C often omits “Comparison with prior,” prompting targeted retraining to bring reports in line with the standard.
The Role of Teleradiology in Multi Branch Practices
Even with strong RIS–PACS foundations and standardized reporting tools, multi-branch hospitals often face spikes in case volumes, subspecialty shortages, or geographic gaps in expertise. This is where teleradiology services play a vital role. They allow hospitals to share cases across locations or outsource to trusted partners while ensuring reports remain uniform in structure and terminology.
1. Cross-Location Reporting Support
Teleradiology enables radiologists in one branch to seamlessly read studies from another branch without delay. A CT done in a smaller facility can be reported by a subspecialist at the main hospital, with the final report following the same standardized template. This ensures that quality is not compromised by branch size or available expertise.
2. Handling Overflow While Keeping Reports Standardized
Multi branch radiology networks often see fluctuating workloads. During peak hours, excess studies can be routed to other branches or external radiologists. When supported by structured templates and integrated RIS–PACS systems, these overflow reports still follow the same format, preventing fragmentation of reporting styles.
- Uniform style guides ensure outsourced reports mirror internal standards.
- Cloud PACS integration allows specialists to access studies instantly.
- Central governance guarantees that reports, no matter the origin, remain consistent.
Mediog’s Contribution to Standardized Reporting
For hospitals and diagnostic networks, ensuring consistency across branches is not only a clinical necessity but also a reputational one. Mediog addresses this challenge by providing a single platform where imaging, reporting, and collaboration converge.
- Unified RIS–PACS Framework: Mediog integrates patient data, imaging, and reporting templates across all branches, ensuring that every radiology report follows the same structure.
- Cloud Accessibility: Reports and images are available securely across locations through Mediog’s cloud PACS, allowing radiologists to review studies in real time.
- Teleradiology-Ready: Mediog supports cross-branch and external reporting, giving hospitals the flexibility to handle overflow without losing consistency.
- AI-Assisted Reporting: With built-in AI features, Mediog accelerates draft generation and enforces uniform terminology, minimizing human variation.
- Governance and Auditing Tools: Administrators can monitor report quality across branches, identify gaps, and ensure adherence to standards.
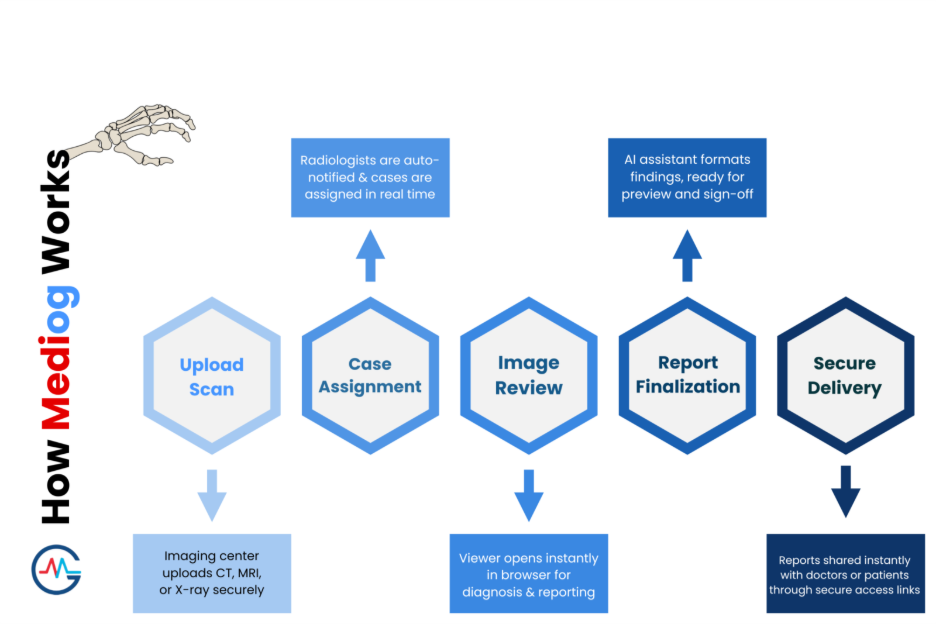
How Mediog maintains the Workflow
In practice, this means a hospital group can run ten branches but still deliver reports with a single, unified “voice.” Radiologists save time, clinicians gain clarity, and patients receive consistent information no matter where they are treated.
Conclusion
For decision-makers, the priority is not just efficiency but also reliability across every branch. Standardized radiology reporting is the foundation of that trust. Hospitals that invest in integrated RIS–PACS systems, structured templates, and teleradiology-enabled workflows will avoid fragmentation and strengthen collaboration. The question is no longer whether to standardize, but how quickly to implement it. Leaders who act early will position their networks as consistent, credible, and future-ready in patient care delivery.
###